Evaluation And Management of Status Epilepticus in Children
Introduction
Status epilepticus (SE) is the most common childhood neurological emergency. Practically, SE is defined as any child presenting convulsing to a healthcare facility or having repeated seizures without regaining of consciousness in between. The International League Against Epilepsy (ILAE) defines SE in terms of time points (t1 and t2) (Table 1).
TABLE 1: Status epilepticus (SE) in terms of time points (t1 and t2). | ||
Type of SE | Time beyond which if seizures persist, patient is considered in SE (t1) | Time after which persistent seizures have long-term consequences (t2) |
Generalized convulsive SE | 5 minutes | 30 minutes |
Focal status with impaired consciousness | 10 minutes | >60 minutes |
Etiology
Etiology may be known or unknown:
· Known (symptomatic):
•• Acute (stroke, toxicity, derangements in serum electrolytes and blood glucose, trauma, hypoxia, febrile seizures, neuroinfections, and inborn errors of metabolism)
•• Remote (brain scars due to above causes, genetic, brain malformations, etc.)
•• Progressive (neurodegenerative disorders and tumors)
•• Known cases of epilepsy: Poor drug compliance or by nature drug-resistant epilepsies such as Lennox–Gastaut syndrome and Dravet syndrome
· Unknown cause: Entities like new-onset refractory status epilepticus (NORSE), a subset of which is febrile infection-related epilepsy syndrome (FIRES)
Management
Status epilepticus is a life-threatening emergency. To improve outcomes, each unit should have a fixed protocol and team members should be familiar with their roles. Diagnosis and management should proceed together. A quick focused history and examination help to search for etiology, which helps in streamlining diagnostic work- up.
Prehospital Management (Home or Clinic)

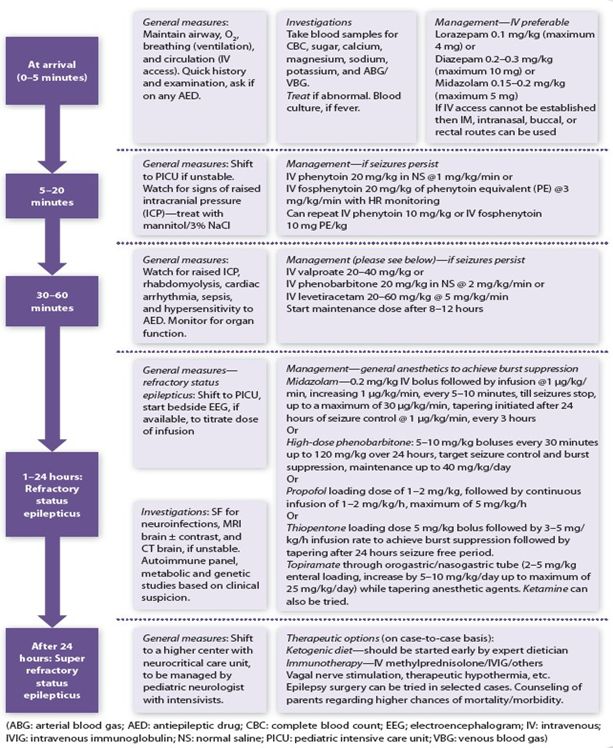
In-hospital Management
Special Points
· All caregivers of children with seizures should be taught first aid including recovery position and use of rescue medications.
· These three drugs are not preferred in a particular sequence. Avoid phenobarbitone if facility for mechanical ventilation is not available; avoid valproate if suspected inborn error of metabolism or liver dysfunction (levetiracetam is the preferred drug in such cases).
· In known cases of epilepsy with breakthrough seizures (on phenytoin ≤6 mg/kg/day, phenobarbitone ≤5 mg/kg/day, valproate ≤30 mg/kg/day or levetiracetam ≤30 mg/kg/day), give half the maintenance dose. For larger doses avoid loading and give the maintenance dose.
Outcome
Mortality in acute phase is seen in 10–20 %. Around 15–56% show long-term cognitive and motor disability.
Conclusion
A structured and systematic approach should be followed for treatment of SE, with the role of individual team members well-specified beforehand, as …. Time is Brain!
Further Reading
· Gulati S, Sondhi V, Chakrabarty B, Jauhari P, Lodha R, Sankar J. High dose phenobarbitone coma in pediatric refractory status epilepticus; a retrospective case record analysis, a proposed protocol and review of literature. Brain Dev. 2018;40:316-24.
· McKenzie KC, Hahn CD, Friedman JN. Emergency management of the paediatric patient with convulsive status epilepticus. Paediatr Child Health. 2021;26:50- 66.
· McTague A, Martland T, Appleton R. Drug management for acute tonic-clonic convulsions including convulsive status epilepticus in children. Cochrane Database Syst Rev. 2018;1:CD001905.
· Mishra D, Sharma S, Sankhyan N, Konanki R, Kamate M, Kanhere S, et al. Consensus Guidelines on Management of Childhood Convulsive Status Epilepticus. Indian Pediatr. 2014;51:975-90.
· Trinka E, Cock H, Hesdorffer D, Rossetti AO, Scheffer IE, Shinnar S. A definition and classification of status epilepticus—Report of the ILAE Task Force on Classification of Status. Epilepsia. 2015;56: 1515-23.
References
- Gulati S, Sondhi V, Chakrabarty B, Jauhari P, Lodha R, Sankar J. High dose phenobarbitone coma in pediatric refractory status epilepticus; a retrospective case record analysis, a proposed protocol and review of literature. Brain Dev. 2018;40:316-24.
- McKenzie KC, Hahn CD, Friedman JN. Emergency management of the paediatric patient with convulsive status epilepticus. Paediatr Child Health. 2021;26:50- 66.
- McTague A, Martland T, Appleton R. Drug management for acute tonic-clonic convulsions including convulsive status epilepticus in children. Cochrane Database Syst Rev. 2018;1:CD001905.
- Mishra D, Sharma S, Sankhyan N, Konanki R, Kamate M, Kanhere S, et al. Consensus Guidelines on Management of Childhood Convulsive Status Epilepticus. Indian Pediatr. 2014;51:975-90.
- Trinka E, Cock H, Hesdorffer D, Rossetti AO, Scheffer IE, Shinnar S. A definition and classification of status epilepticus—Report of the ILAE Task Force on Classification of Status. Epilepsia. 2015;56: 1515-23.