Fasting levels are lower when compared to the corresponding post-prandial levels from the same site.
In the fasting state, venous= capillary values but in the post prandial state, venous is less thancapillary values as the rise in posr prandial insulin pushes glucose into tissues.
Whole blood glucose values are lower than plasma values as red cell glucose concentration is lowerthan plasma.
In the post prandial state, capillary whole blood and venous plasma values are the same For glucose, 1 mmol/L =18 mg%
CRITERIA FOR TESTING FOR DM
1. Symptomatic patients (Polyuria, polydipsia, polyphagia, unexplained weight loss).
2. All individuals at age 45 or older. If results are normal, they should be repeated atappropriate intervals e.g. 1/year or at 3 year intervals.
3. Test should be done in younger individuals if:
I. They are obese (BMI >30 for men and >28.6 for women)
II. First degree relative with DM
III. Are members of high risk ethnic population
IV. Are hypertensive (BP > 140/90 mm of Hg)
V. Have HDL cholesterol of less than/=35mg% and/or triglycerides of more than/=250mg%
VI. On a previous testing had IGT (Impaired glucose tolerance) or IFG (Impaired fastingglucose)
VII. Presenting with acute MI/stroke, peripheral neuropathy, proteinuria, peripheralvascular disease.
4. In pregnancy if GDM (Gestational DM) is suspected- Criteria for diagnosing Diabetes Mellitus
American Diabetes Association: Clinical Practice Recommendations 2002
1. Symptoms of diabetes plus casual plasma glucose concentration >200mg/dL (11.1 mmol/l).Casual is defined as any time of the day without regard to time since last meal. The classic symptoms of DM include polyuria, polydipsia and unexplained weight loss.
OR
2. FPG > 126 mg/dl (7.0 mmol/l). Fasting is defined as no calorie intake for at least 8 hours.
OR
3. 2-h PG >200mg/dl (11.1 mmol/l) during an OGGT #. The test should be performed as described by WHO, using a glucose load containing the equivalent of 75 g anyhydrousglucose dissolved in water.
In the absence of unequivocal hyperglycemia with acute metabolic decompensation, these criteria should be confirmed by repeat testing on a different day. The third measure (OGGT- oral glucose tolerance) test is not recommended for routine clinical use.
#Values for diagnosing DM and other forms of hyperglycemia based on OGTT (75gm of glucose)
(Ref: 1998 WHO consultation group)
CMCH laboratory values correspond to the venous plasma values. Glucose concentrations should NOT be measured on serum unless red cells are immediately removed, otherwise glycolysis will result in an unpredictable underestimation of the true concentrations. For epidemiological purpose of screening for DM, 2-h post glucose load value exceeding 200mg% in venous plasma is sufficient asmentioned above.
OGTT (75 gm of glucose) Ref : 1998 WHO consultation group
Fasting values reflect ENDOGENOUS glucose production Post prandial values reflect EXOGENOUSintake
AIMS OF TREATMENT IN DIABETES MELLITUS
· Save life
· Alleviate symptoms
· Prevent long term complications
· Reduce risk factors- Smoking, HT, Obesity, Hyperlipidemia
· Educate and encourage self management
TARGETS FOR CONTROL
ADA Recommendations 2006
BMI <27
Lipids:
LDL Cholesterol <100 mg% HDL Cholesterol >45 mg% Trigycerides<150 mg%
Blood Pressure < 130 /80 mm Hg
Glucose: Plasma Whole Blood
Fasting 90 – 130 mg% 80 – 120 mg%
Bedtime 110 – 150 mg% 100 – 140 mg%
HbA, C 7%
Less stringent goals are appropriate for the very old, those with limited life expectancy and those with frequent hypoglycemic attacks. Elevated post challenge (2hour OGTT) has been associated withincrease cardiovascular risk irrespective of the value of fasting plasma glucose. There are pharmacological agents that primarily modify post prandial glucose and monitoring post prandial glucose 2 hours after a meal with an aim to reduce it to < 180mg% lowers HbA,C in those with high HbA,C and normal fasting glucose. However, there are no studies are available to show the efficacy of such a regimen to reduce complications in those with either Type I or Type II Diabetes mellitus.
Specify therapy for Post Prandial Hyperglycemia:
· Metformin
· Repaglinide
· Acarbose
· Insulin lispro
INSULIN THERAPY IN DIABETES LELLITUS
Insulin can be bovince porcine, human. Human insulin is structurally similar to the psysiological insulin secreted by the human pancreas, whereas porcine insulin differs from human by 1 amino-acid and bovine differs from human by three amino-acids.
Human insulins produced by genetic re-engineering techniques are now used universally after reduction in prices. However, monocomponent bovine and porcine insulin are still available for verypoor patients.
Strength: The commonly available strengths are – 40 IU/ml and 100IU/ml. It is important to use the syringes corresponding to the strengths of insulin to avoid hypoglycaemia.
Storing: Can be stored temperatures of 2-8 °C (first shelf of the refrigerator) if needed to store for long periods. It can however be kept at room temperature (Indian conditions), away from sunlightfor about 4-6 weeks with no apparent loss in biological activity.
Purity: Categorised into-
a) Highly purified insulin: with < 10ppm of pro-insulin like substances.
b) Monocomponent insulin: with < 1ppm of pro-insulin like substances.
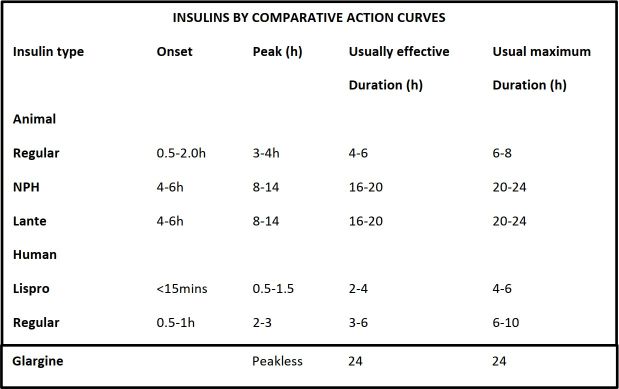
Newer insulin: these are insulin analogues: Lispro, Glargine
Time duration and effect:
References
No references available